
Safety in Pediatric Orthopedics
Advances in Pediatric Orthopedics
A Steadfast Obligation to Safety in Spine Surgery
What began as a concern a number of years ago about a surgical complication observed by Michael G. Vitale, MD, inspired a transformational initiative in spine deformity surgery safety that is today unparalleled. In 2014, Dr. Vitale and colleagues in the field launched The Safety in Spine Surgery Project (S3P) to improve the safety of surgical treatment of spine problems in adult and pediatric populations by developing best practice guidelines at its foundation.
“This initiative is about how we can collectively make spine surgery safer together,” says Dr. Vitale, who is Chief of Pediatric Spine and Scoliosis Surgery in the Department of Orthopedic Surgery at NewYork-Presbyterian/Columbia University Irving Medical Center. He also serves as Vice Chair, Quality and Strategy, Orthopedic Surgery, and the Ana Lucia Professor of Pediatric Orthopedic Surgery and Neurosurgery at Columbia. “Key to this goal was the establishment of an annual spine safety summit. For a number of years, we held the program in New York with standing room only. The meeting sold out six years in a row. In the last few years, we began simulcasting the program because the demand was so high.”
“During the last two years, S3P offered virtual webinars, and importantly with regard to scale of messaging, the leadership mobilized a very large social media awareness effort,” adds Dr. Vitale. “Last year, there were 225,000 engagements around this concept of safety in spine surgery with all the major organizations – Scoliosis Research Society, Pediatric Orthopedic Surgery of North America, and study groups – jumping on board and helping to boost that messaging.”
Every year, the meeting focuses on developing a best practice guideline for a specific area in spine surgery, ranging from how to avoid wrong site surgery, responding after loss of intraoperative neuromonitoring signals in the operating room, implementing halo-gravity traction, and preventing infection, as well as those addressing particular issues in complex spine deformity surgery. This is accomplished through expert panels and a formally derived consensus process, the Delphi process. The resulting guidelines have led to some of the most widely cited publications in this field.
“These panels are comprised of thought leaders who are deeply committed and have carefully considered how to make spine surgery safer,” says Dr. Vitale. “They are a group of people representing not only the spinal deformity space, but also cervical spine, degenerative disease, and adult and pediatric minimally invasive surgery, and we continue to broaden our audience around different areas in spine surgery. When we get together, we share methods we are doing differently and come up with a product that's better than the sum of its parts.”
Recent Studies Address Neurological Events and Surgical Site Infections
During the past year, Dr. Vitale, his colleagues at Columbia, and members of S3P and other specially convened expert panels have continued developing best practice guidelines on a number of critical safety issues that continue to confront spine surgeons. Their efforts provide the surgical team with resources that can help drive decisions in unexpected events and optimally preserve the neurological function of patients and curtail the incidence of surgical spine infections.
Neurological Events
In 2014, Dr. Vitale and his colleagues on the S3P expert panel developed the organization’s first formal guidelines, which targeted responding to intraoperative neuromonitoring changes in the operating room. The resulting paper, published in the September 2014 issue of Spine Deformity, was the most widely cited paper in the field. These guidelines have just been expanded upon by Dr. Vitale, Lawrence G. Lenke, MD, Surgeon-in-Chief and Co-Director of Och Spine at NewYork-Presbyterian, and 13 other experienced spinal deformity surgeons across the country. The study team further developed the original consensus-based best practice guidelines to optimize the approach to intraoperative neuromonitoring events associated with “high-risk” spinal deformity surgery. This set of guidelines, published in the July 2022 issue of Spine Deformity, included a response algorithm; ongoing considerations of etiology – systemic, destabilization/
In a companion paper, published in the same issue of Spine Deformity, the expert panel focused on parameters that constitute elevated risk during spinal deformity surgery and potential preventative strategies that may minimize the risk of intraoperative neuromonitoring events and postoperative neurological deficits. The panel identified and achieved consensus on 22 determinants of high-risk items, incorporating 8 patient factors, 8 curve and spinal cord factors, and 6 surgical factors, as well as 21 preoperative (4), intraoperative (14) and postoperative (3) preventative strategies.
Surgical Site Infections
Faced with surgical site infections (SSI) that continue to prevail even with numerous measures developed and implemented to reduce their incidence, Dr. Vitale, Dr. Lenke, along with their Columbia colleagues in the Department of Orthopedic Surgery and at six other major orthopedic centers across the country, came together to develop a prediction model that could quantify the risk of SSI for individual pediatric spinal deformity patients.
Their study included 3,092 spinal deformity surgeries of which there were 132 cases (4.3 percent) of SSI. The final prediction model contained 9 variables based on their ability to predict SSI within 90 days postoperatively:
Patient Characteristics
- Overweight or obese body mass index (BMI)
- Neuromuscular etiology
- American Society of Anesthesiologists (ASA) grade >2
- Non-ambulatory status
- Abnormal hemoglobin level
Surgical Factors
- Revision surgery
- Pelvic instrumentation procedure
- Procedure time ≥7 hours
Hospital Factor
- <100 spine surgical cases per year per institution
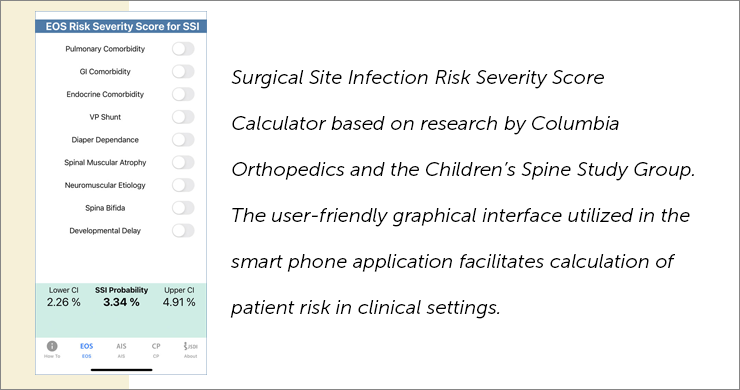
The authors note that the validated calculator enables the surgical team to identify high-risk patients, thereby providing the opportunity to address modifiable risk factors prior to surgery and increase vigilance of the particular surgical factors that increase the risk for SSI.
The Bigger Picture: Preventable Patient Harm
“The majority of complications we see are related to system failures,” notes Dr. Vitale. “I think we under-appreciate the reality that there is an entire episode of care that starts before surgeons enter the OR, whether it relates to skin prep or antibiotics, as examples, but also formal discussion about potential risks before the surgery. If you align your processes, you make it much less likely for the wrong problem to propagate through the system.”
See Complete Article
Read More
- Establishing consensus: determinants of high-risk and preventative strategies for neurological events in complex spinal deformity surgery. Iyer RR, Vitale MG, Fano AN, Matsumoto H, Sucato DJ, Samdani AF, Smith JS, Gupta MC, Kelly MP, Kim HJ, Sciubba DM, Cho SK, Polly DW, Boachie-Adjei O, Angevine PD, Lewis SJ, Lenke LG. Spine Deformity. 2022 Jul;10(4):733-744.
- Development of consensus-based best practice guidelines for response to intraoperative neuromonitoring events in high-risk spinal deformity surgery. Lenke LG, Fano AN, Iyer RR, Matsumoto H, Sucato DJ, Samdani AF, Smith JS, Gupta MC, Kelly MP, Kim HJ, Sciubba DM, Cho SK, Polly DW, Boachie-Adjei O, Lewis SJ, Angevine PD, Vitale MG. Spine Deformity. 2022 Jul;10(4):745-761.
- Best Practices in Intraoperative Neuromonitoring in Spine Deformity Surgery: Development of an Intraoperative Checklist to Optimize Response. Vitale MG, Skaggs DL, Pace GI, Wright ML, Matsumoto H, Anderson RC, Brockmeyer DL, Dormans JP, Emans JB, Erickson MA, Flynn JM, Glotzbecker MP, Ibrahim KN, Lewis SJ, Luhmann SJ, Mendiratta A, Richards BS 3rd, Sanders JO, Shah SA, Smith JT, Song KM, Sponseller PD, Sucato DJ, Roye DP, Lenke LG. Spine Deformity. 2014 Sep;2(5):333-339.
- A Clinical Risk Model for Surgical Site Infection Following Pediatric Spine Deformity Surgery.
Matsumoto H, Larson EL, Warren SI, Hammoor BT, Bonsignore-Opp L, Troy MJ, Barrett KK, Striano BM, Li G, Terry MB, Roye BD, Lenke LG, Skaggs DL, Glotzbecker MP, Flynn JM, Roye DP, Vitale MG. The Journal of Bone Joint Surgery. American volume. 2022 Feb 16;104(4):364-375. - Safety Does Not Happen by Accident: Preventing Human Error Through High-Reliability Practices. Vitale MG, Raman DL. Journal of Pediatric Orthopedics. 2022 May-Jun 01;42(Suppl 1):S35-S38.
- The Safety in Spine Surgery Project
- April 2022 Spine and Safety Conference Videos

 Watch this video introduction by Dr.
Watch this video introduction by Dr. 
